PEN eNews 7(2) September 2017
September 2017 · Volume 7, Issue 2

A lie can travel halfway around the world while truth is putting on its shoes (unknown)
On a recent plane ride for a short family vacation I sat beside a retired nurse. The usual plane-conversation ensued and they asked me what I did. When I said I am a dietitian, they excitedly told me about a family member who was cured of their celiac disease by electrotherapy resulting in the elimination of “parasites that cause celiac disease”. They also used it on the parasites in their grand daughter’s ovaries and now her dysmenorrhea was also cured. Did I know that most disease has a parasitical root?
This was followed mere hours later with a conversation with a friend challenging me about homeopathy. “What’s your problem – while it might not work, homeopathy doesn’t do any harm”.
In the airport, on my way home, my Twitter feed was afire with the GOOP/Dr Jen Gunter exchange. Dr Jen earned Wonder Woman memes (see below) for challenging GOOP’s misinformation and dubious products.
The work I do with Dietitians of Canada and the PEN System requires me to evaluate evidence and sometimes challenge recommendations or opinions. I am constantly reflecting on the best strategies to do this both for my work and in my personal exchanges with family and others.
Different situations may call for different strategies.
If something is clearly “bunk” or nonsense, I think we need to simply and clearly state the truth. Tim Caulfield and Dr Gunter do this really effectively, often on a daily basis. Keep in mind that a “simple” myth is easier to hang on to than an overly complex explanation of the truth. We need to practice converting our complex knowledge of science, nutrition and biochemistry into clear, relatable facts to bust the myths out there. This is hard, and paraphrasing Brandolini’s law: the amount of energy needed to refute nonsense is an order of magnitude bigger than that needed to produce it.
Still, we must persist!
"I think setting the scientific record straight matters. It may not change people's minds tomorrow, but ensuring the facts are out there will make a difference long term," Tim Caulfield in http://www.cbc.ca/news/health/second-opinion170722-1.4215614
For more complex debates, we may need some different strategies, especially when there appears to be some evidence to support either side of the debate. Here are a couple of strategies that I’m trying to use:
- Be critical of weak evidence no matter which side of a debate it supports.
- Be curious, and open to good quality evidence even if it doesn’t support your belief. Knowledge changes as new evidence emerges.
- Try to explain why you believe in something, not just why the other person is wrong.
This article by Nicole Letourneau highlighted the importance of using an evidenced-based approach in those situations. In her article entitled ”Public health at risk when opinion trumps evidence”, she reminds us that good policy relies on good evidence and evidence-based practice encourages us to also consider the context that the evidence will be applied in and to respect patient values.
If you are looking for something interesting to listen to on your next walk or gym workout listen to: Truth and Lies from the TED Radio Hour.
So what did I respond to my recent scenarios?
Well, to my seatmate, I stated up front that I was skeptical of the theory that suggested most diseases result from parasites. I tried to build on their nursing background to discuss how our immune system works, mentioned a couple of diseases that don’t have parasites as a cause (melanoma, macular degeneration) and had a lively conversation about how the placebo effect can make you think the intervention you just paid for “cured you”.
For my friend who was supporting homeopathy, I explained that there was no science behind homeopathy. And that yes, it can cause significant harm if it is used to treat a serious disease instead of a proven therapy. I explained to her that I’m not so worried about the risk of using homeopathy to treat a wart, but what if it is used to treat a high fever in an infant. As a mother herself, the example was relatable for her.
I don’t think I changed the mind of my seatmate, but I know I made an impact on my friend. I’ll take a 50% success rate for now and keep honing my skills at using critical thinking and evidence to bust the nutrition myths when I come across them.
Written by:
Jayne Thirsk RD PhD FDC
Director PEN: Practice-based Evidence in Nutrition®
enews@pennutrition.com
In this issue of PEN eNews 7(2), we:
- Introduce you to our PEN award winners
- Help you avoid falling prey to predatory journals
- Show you how to use PEN to debunk some myths
- Put “P” value in its place
- Introduce you to a family of reviews
- Help you the PES Statements in the Toolkits
- …all this and more in PEN eNews 7(2)!
A Publication of the PEN® System Global Partners, a collaborative partnership between International Dietetic Associations. Learn more about PEN.
What's New in PEN®
Updated Knowledge Pathways
Updated Practice Questions
- Is the nutrition facts/information panel an effective means of communicating nutrition information to consumers?
- To what extent do consumers want, understand and use nutrient content and health claims on packaged food products?
- Why are disordered eating behaviours and eating disorders more prevalent among individuals with type 1 diabetes than their non-diabetic peers?
- Do individuals with type 1 diabetes with an eating disorder or disordered eating have an earlier onset of diabetes complications?
- What is the optimal treatment for adolescent females with type 1 diabetes and eating disorders?
- Is creatine supplementation effective for improving muscular strength or function in individuals with muscle disorders (myopathies)?
- Are males susceptible to eating disorders and, if so, does this vary from eating disorders among females?
- Are there dietary recommendations to correct low blood pressure in individuals with heart failure? Should sodium intake be liberalized to above the recommended intake of 2-3 grams/day?
- Can sodium intake be liberalized in individuals with heart failure (HF) who are residents in long-term care facilities without adversely affecting clinical stability?
- Should individuals with heart failure (HF) abstain from alcohol intake to reduce the progression of HF and/or to reduce the risk of adverse cardiovascular outcomes?
- What is the best approach for planning educational programs to promote adherence to dietary therapies for individuals with heart failure (HF)?
- What are the indications and contraindications for feeding term infants and/or toddlers a lactose-free formula?
-
Are front-of-package (FOP) and point-of-purchase (POP) grocery store food labelling systems effective means of communicating nutrition information to consumers and influencing diet?
Professional Tools
- Food and Nutrition Labelling Evidence Summary
- Infant Nutrition - Infant Formula Evidence Summary
- Omega-3 Fatty Acids and Health
- Diabetes - Eating Disorders Background
- Flavonoid and Fat Content of Chocolate Foods
- Dysphagia Assessment and Management - DC Online Courses
- Musculoskeletal/Connective Tissue Disorders Evidence Summary
- Cardiovascular Disease - Chocolate Evidence Summary
- Cardiovascular Disease - Heart Failure Evidence Summary
- Bone Health Evidence Summary
- Telehealth/Teledietetics Evidence Summary
- Dietitians in Telehealth
- International Nutrition Guidelines Collection for Pregnancy (Prenatal/Antenatal)
- Malnutrition Evidence Summary
- Gastro-oesophageal Reflux Disease in Adults
- Diabetes and Eating Disorders Web Links
- International Society of Sports Nutrition Position Stand
- Responding to Nutrition Misinformation – Toolkit
- Pregnancy Background
- 2016 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult
- Competencies for Dysphagia Assessment and Management in Dietetic Practice
- Fr: Compétences en évaluation et gestion de la dysphagie dans l’exercice de la diététique (Competencies for Dysphagia Assessment and Management in Dietetic Practice)
- Infant Nutrition - Infant Formula Practice Guidance Toolkit
- Pregnancy Practice Guidance Toolkit
- Diet Composition - Alkaline Diet Practice Guidance Toolkit
Trending Topics
New Knowledge Pathways
New Practice Questions
- What is the optimal treatment strategy for individuals with type 2 diabetes and eating disorders?
- Should commercially available chocolate or cocoa products be recommended to healthy adults to reduce the risk of cardiovascular disease (CVD)?
- Should adults with malnutrition or at risk of malnutrition be recommended nutrition intervention in hospital?
- Is modifying the organization of nutrition care in hospitals (e.g. to include nutrition protocols, nutrition care teams) recommended for the prevention and treatment of malnutrition in adults?
- Are interventions to decrease dietary cholesterol intake (e.g. restricting eggs) recommended for the secondary prevention of cardiovascular disease (CVD)?
- Are interventions to decrease dietary cholesterol intake (e.g. restricting eggs) recommended for the primary prevention of cardiovascular disease (CVD)?
- Are there specific characteristics of male athletes that may increase their risk of disordered eating?
- What are some characteristics or behaviors in males that may contribute to the risk of developing eating disorder, or worsen disordered eating behaviors?
- Does dysphagia assessment and management fall within a dietitian’s scope of practice?
Client Tools
- Healthy Snack Ideas: Type 2 Diabetes – Adapted for Latin American Communities
- Healthy Snack Ideas: Type 2 Diabetes - Adapted For South Asian Communities
- Fr: Healthy Snack Ideas: Type 2 Diabetes - Adapted for African and Caribbean Communities
- Healthy Snack Ideas: Type 2 Diabetes - Adapted for Chinese Communities
- Ch: Healthy Snack Ideas: Type 2 Diabetes: Adapted for Chinese Communities
- Pun: Healthy Snack Ideas: Type 2 Diabetes - Adapted For South Asian Communities
- Mediterranean Diet Sample Menu (1500 kcal)
- Fr: Exemples de menu du régime méditerranéen (1500 kcal) (Mediterranean Diet Sample Menus 1500 kcal)
- Healthy Eating While Spending Less - Adapted for Chinese Communities
- Ch: Healthy Eating While Spending Less - Adapted for Chinese Communities
- Healthy Snacks for Adults - Adapted for Chinese Communities
- Healthy Snacks for Adults - Adapted for Latin American Communities
- Healthy Snacks for Adults - Adapted for African and Caribbean Communities
- Ch: Healthy Snacks for Adults - Adapted for Chinese Communities
- Sp: Healthy Snacks for Adults - Adapted for Latin American Communities
- Healthy Snacks for Adults - Adapted for South Asian Communities
- Ur: Healthy Snacks for Adults - Adapted for South Asian Communities
- Tam: Healthy Snacks for Adults - Adapted for South Asian Communities
- Pun: Healthy Snacks for Adults - Adapted for South Asian Communities
- Diabetes and Mental Health
- Fr: Diabète et snaté mentale (Diabetes and Mental Health)
- Fr: Votre glycémie : hypoglycémie et hyperglycémie (Lows and Highs: Blood Glucose Levels)
- Eating Disorders
- Fr: Les troubles de l’alimentation (Eating Disorders)
- Eating Disorders – Your Guide
- Eating Well With Neutropenia: A Guide for People With Blood Cancer
- Fr: Healthy Snacks for Adults - Adapted for African and Caribbean Communities
- Hin: Healthy Snack Ideas: Type 2 Diabetes - Adapted For South Asian Communities
- Guj: Healthy Snack Ideas: Type 2 Diabetes - Adapted For South Asian Communities
- Hin: Healthy Snacks for Adults - Adapted for South Asian Communities
- Guj: Healthy Snacks for Adults - Adapted for South Asian Communities
- Mediterranean Diet Sample Menu (2000 kcal)
- Fr: Exemples de menu du régime méditerranéen (2000 kcal) (Mediterranean Diet Sample Menus 2000 kcal)
How do I… find PES Statements in PEN® Practice Guidance Toolkits?
Kerri Staden BSc, RD Dietitians of Canada
PEN® Resource Managers
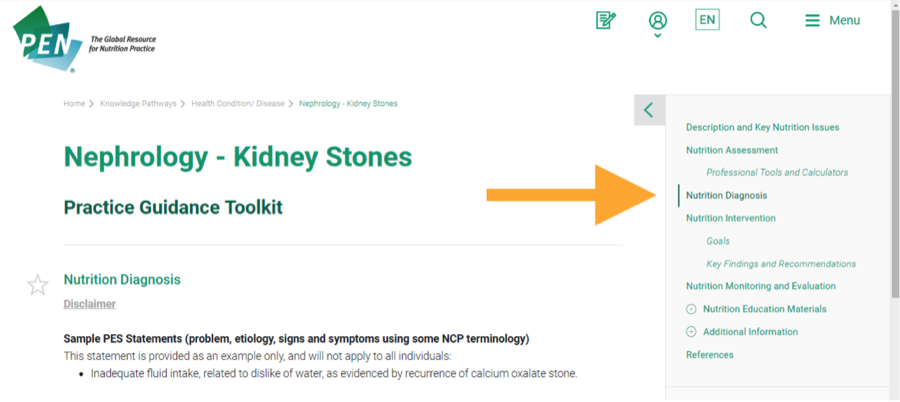
Participants from focus groups held at the Dietitians of Canada conference in colourful St. John’s Newfoundland, Canada found the Nutrition Care Process (NCP) sections within PEN Toolkits useful, especially the Nutrition Diagnosis section that contains examples of PES (problem, etiology, signs & symptoms) statements.
The NCP is a framework that follows NCP terminology developed by the Academy of Nutrition and Dietetics (AND). It is used to improve the consistency, communication, coordination and quality of nutrition care, along with the predictability of the nutrition care outcomes (1).
PEN toolkits (2) contain the same sections that are found in the NCP: Nutrition Assessment; Nutrition Diagnosis; Nutrition Intervention; and Nutrition Monitoring and Evaluation. In addition, toolkits contain client education materials and clinical guidelines sections.
PES statements
A PES statement, or a nutrition diagnosis statement, is a sentence describing the specific nutrition problem, its cause(s), and the evidence or proof of the problem (3). Statements are generally written as: The problem (i.e. swallowing difficulty), ‘is related to’ an etiology (i.e. a stroke) ‘as evidenced by’ specific signs and symptoms (i.e. coughing after drinking water from a cup).
Here’s an example from the Nephrology - Kidney Stones Toolkit:
PES Statement: Inadequate fluid intake, related to dislike of water, as evidenced by recurrence of calcium oxalate stone.
For more information:
1. Nutrition Care Process and Terminology Background
2. Listing of Practice Guidance Toolkits in the PEN System.
3. eNCPT Tutorials
As always, we welcome your feedback.
PEN® Resource Managers:
Jane Bellman MEd, RD
Kerri Staden BSc, RD
jane.bellman@dietitians.ca
kerri.staden@dietitians.ca
Don’t Fall Prey to Predatory Journals
A PEN Community member recently flagged a journal on our LinkedIn platform that prompted us to investigate and reflect on predatory journals.
What are predatory journals?
“Predatory journals” are produced by “predatory publishers” who oftenprey on researchers and trainees to submit manuscripts through aggressive marke
 ting campaigns (1). Unlike legitimate journals, they send out mass email messages offering ”rapid peer-review” and publication, but without adhering to scholarly publishing standards or external peer review (2). Most of these “journals” (essentially websites) are in low and middle-income countries (but often use addresses in the US and UK), and confuse readers by creating journal and publisher names / logos that are very similar to legitimate journals. They may claim to be indexed, but are not indexed in any legitimate electronic databases (such as PubMed). The World Association of Medical Editors (WAME) has issued a statement against predatory or pseudo-journals that publish open access papers for a fee paid by the author, but without regard to the scientific quality of these papers (1).
ting campaigns (1). Unlike legitimate journals, they send out mass email messages offering ”rapid peer-review” and publication, but without adhering to scholarly publishing standards or external peer review (2). Most of these “journals” (essentially websites) are in low and middle-income countries (but often use addresses in the US and UK), and confuse readers by creating journal and publisher names / logos that are very similar to legitimate journals. They may claim to be indexed, but are not indexed in any legitimate electronic databases (such as PubMed). The World Association of Medical Editors (WAME) has issued a statement against predatory or pseudo-journals that publish open access papers for a fee paid by the author, but without regard to the scientific quality of these papers (1). For several years, Jeffrey Beall from the University of Colorado Denver, compiled annual lists of “potential, possible, or probable” predatory publishers, with almost 1300 predatory journals listed in January 2017 (3)! The list is no longer being kept. Beall shut down the blog in January 2017 due to pressure from the university where he was employed and fear of losing his job (4).
Are all open access journals predatory journals?
Although predatory journals have open access articles, predatory publishing should not be confused with open access publishing (refer to PEN eNews: What’s the buzz about open-access journals?). The Directory of Open Access Journals (DOAJ) identifies legitimate open access journals that use a quality control system (i.e. peer-review with an editor and editorial board). Legitimate open-access journals should also belong to the Open Access Scholarly Publishers’ Association (OAS-PA).How can predatory journals be stopped?
Unfortunately these journals continue to proliferate likely due to the desperation of researchers to quickly and continually publish in order to advance their careers. This makes it difficult for readers (including the media) to identify legitimate research in a high-quality journal. Stopping predatory journals requires a collaborative effort to raise awareness of the problem and to promote publication literacy (5). Some resources to help identify trusted journals are:
- “Think-Check-Submit” initiative provides an easy-to-use checklist to investigate whether a journal can be trusted.
- WAME provides guidance to editors, researchers, funders, academic institutions and other stakeholders to distinguish predatory journals from legitimate journals (1).
References
- Laine, C, Winker MA. Identifying predatory or pseudo-journals. World Association of Medical Editors (WAME); February 15, 2017 [cited 2017 Aug 1]. Available from: http://www.wame.org/identifying-predatory-or-pseudo-journals
- Khan F, Moher D. Predatory Journals: do not enter. University of Ottawa Journal of Medicine. January 2017(1):1-5 [cited 2017 Aug 1]. Available from: https://uottawa.scholarsportal.info/ojs/index.php/uojm-jmuo/article/view/1755
- Voutier C. Royal Melbourne Hospital - Exploring the Evidence Base. Beall’s list of predatory publishers; Jan. 2017 [cited 2017 Aug 1]. Available from: https://clinicallibrarian.wordpress.com/2017/01/23/bealls-list-of-predatory-publishers/
- Beall J. What I learned from predatory publishers. Biochem Med (Zagreb). 2017 Jun 15; 27(2): 273–278. doi: 10.11613/BM.2017.029. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5493177/
- Clark J, Smith R. Firm action needed on predatory journals. BMJ. 2015 Jan 16;350;h210. Citation available from: https://www.ncbi.nlm.nih.gov/pubmed/25596387
Written by:
Dawna Royall MSc, RD, FDC
PEN® Senior Evidence Analyst
Editor, Canadian Journal of Dietetic Practice and Research
PEN Evidence-Based Practice Prize Winners for 2017
 |
| Sarah Andersen APD - Nutrition Support Protocols for Stem Cell Transplant |
 |
| Adrienne Forsyth APD on behalf of the Mental Health Interest Group |
PEN Celebrates More Contributors
 |
| Becky Blair, RD MSc Public Health Nutritionist, Child Health Program |
- education/professional enhancement,
- career achievements,
- initiative/innovation and
- leadership in the profession of dietetics."
Among Dawna’s many accomplishments, she has authored DC role papers which captured the voice of Primary Care dietitians across the country; she has conducted systematic evidence reviews to
 |
Dawna Royall MSc RD FDC |
PEN® Tools to support your PEN® experience!
Need a quick introduction or refresher on how to get the most out of the PEN® System? We’ve got just the resources… PEN® Video Tutorials and ToursWhether you are new to the PEN System or a seasoned user, take a few minutes to learn more about all the PEN System has to offer!
From the PEN Menu choose:
PEN® Tours and Video Tutorials
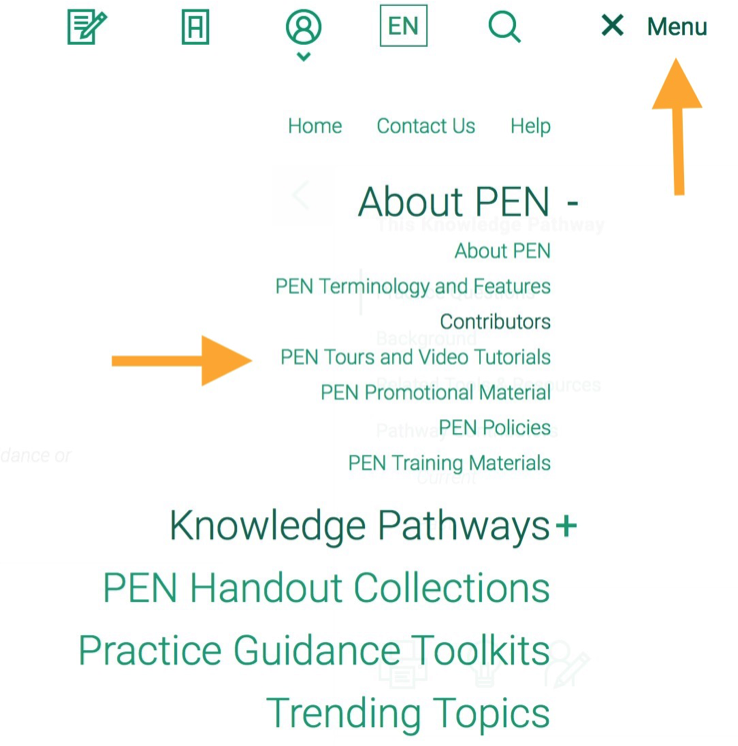
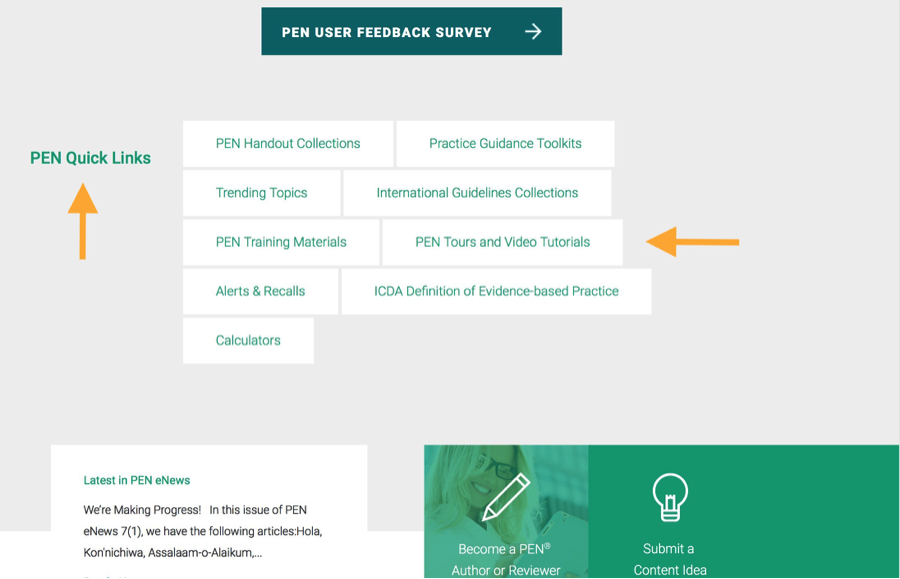
OR - From the PEN Home page, once logged into PEN, go to PEN Quick Links in the middle of the page and choose PEN Tours and Video Tutorials:
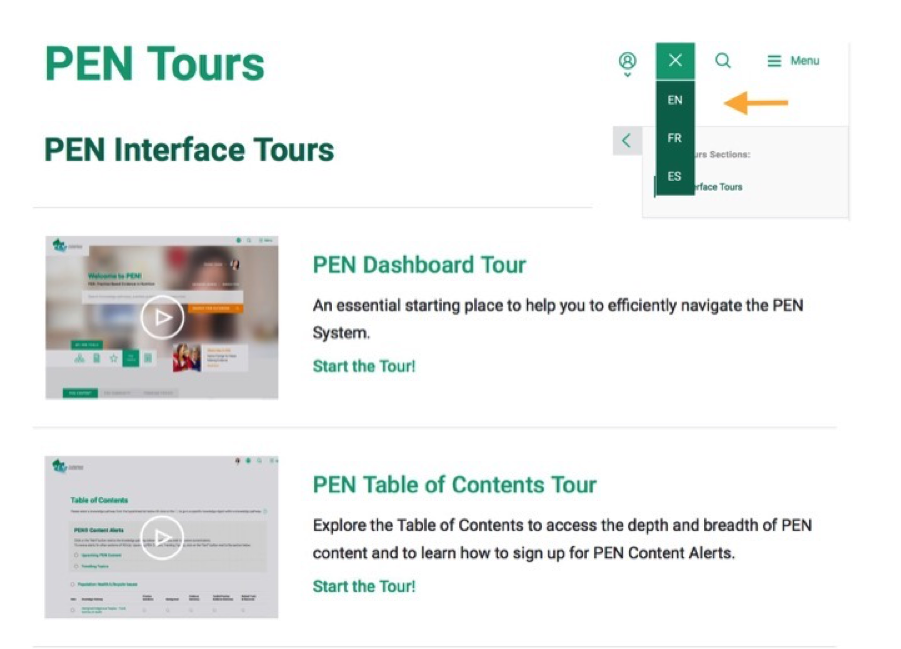
PEN® Tours
There are two very short PEN Tours available:
- PEN Dashboard Tour and
- PEN Table of Contents Tour
Depending on your language of navigation in PEN your Tour will be in the same language (orange arrow).
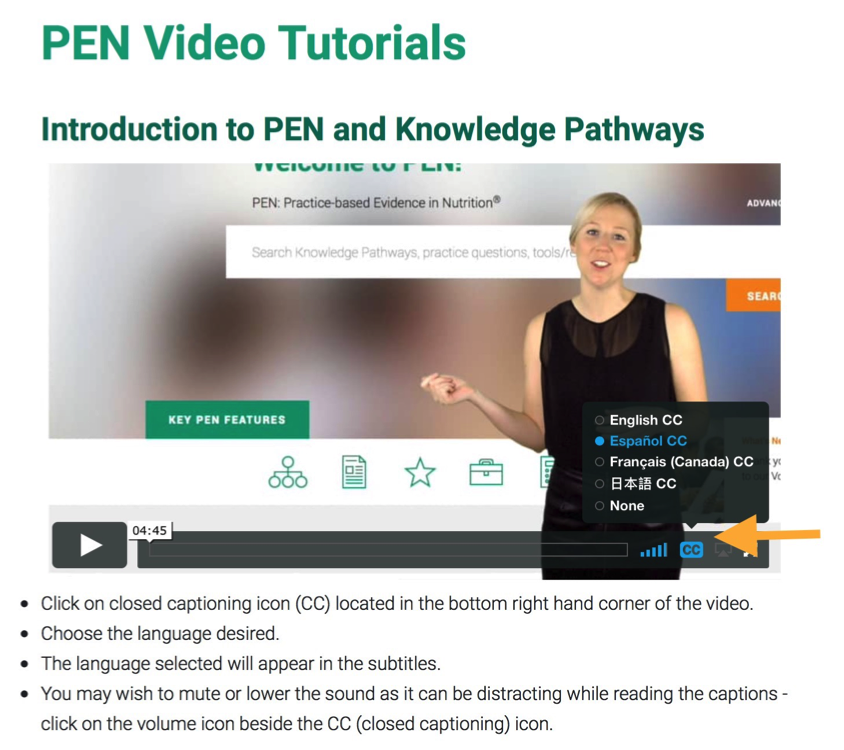
PEN® Video Tutorials
Four short, less than 5 minutes each, PEN video tutorials are available:
-
Introduction to the PEN System
-
Getting to Know Knowledge Pathways
-
Introduction to Practice Guidance Toolkits
- Using PEN Tools and Resources
They are available in English with close captioning (CC) subtitles in French, Spanish and Japanese for our growing international PEN community. Depending on your language of navigation in PEN you will see the titles of the video tutorials in the same language.
By clicking on the blue CC as in the screenshot below (orange arrow) you can access the sub-titles in the language you desire.
We hope these tools will help support your PEN® experience!
Written by:
Beth Armour PDt MEd
PEN® Content Manager
beth.armour@dietitians.ca
We asked, you gave feedback, and we are listening!
In the spring of 2017 the PEN team decided it was time to get feedback from our users on the tools used to present the evidence in PEN with the objective of making changes based on the feedback. In addition to the Contact Us on the PEN website, where PEN users can always give feedback, we created three opportunities for user feedback. Here is a sneak peek at what we have learned so far.
In addition to the Contact Us on the PEN website, where PEN users can always give feedback, we created three opportunities for user feedback. Here is a sneak peek at what we have learned so far.
PEN User Feedback Survey
PEN User Feedback Survey - has been linked from the Home page of the PEN website since May 2017. At the time of writing we have had more than 100 responses from all partner associations and other international PEN users.
Some preliminary results:
- while most usually find what they are looking for there are a number of users looking for a topic that is not on PEN yet
- some have indicated the questions are too specific and others indicate they are not specific enough
- some content is out of date and we are working on that….. there are over 1100 questions in PEN – that’s a lot of updating!
- those who look at some of our evidence tools – e.g. Evidence Statements, Evidence Summaries, Practice Guidance Toolkits and Trending Topics find them useful
- a number of users do not find the tools and resources they are looking for, the PEN team have begun to look at keywords used and the search function
- when asked if they could change one thing on the PEN website we received a number of suggestions from a PEN app, better searching / navigation to more Trending Topics
- finally when asked if they would recommend PEN to a colleague 85% said Yes!
Thank you to those who took the time to complete the survey. Watch for future articles in PEN eNews on how we are using your feedback.
PEN User Focus Groups
PEN User Focus Groups - two were held at the Dietitians of Canada conference in St. John’s, Newfoundland in June with a total of 11 people who were assigned to do some pre-session homework. There were great discussions and feedback on Related Tools and Resources / Third Party Handouts, PEN Handouts, Toolkits, Evidence Summaries, Videos, Calculators, Trending Topics. Highlights include:
- General – all participants said that until they had completed the focus group pre-work assignment, they weren’t aware of all of the PEN features.
- Evidence Summaries - all mentioned they were valuable.
- PEN developed handouts (Canada) - recommended a shorter, lower literacy version of some of them.
- Trending Topics – very well liked and wanted more, although the separate classification of articles weren’t well understood. As a result of the feedback, all articles will now simply be called Trending Topics.
- Toolkits were found to be particularly useful for new dietitians and for all dietitians when writing problem, etiology, signs and symptoms statements (PES).
- Searching for tools and resources – participants aren’t always able to find what they are looking for. We are looking at number of strategies to help you find what you need.
PEN Pop-up Surveys
PEN Pop-up Surveys just became active at the time of writing. They can be found on certain Toolkits and Background documents that are frequently used. The survey is short – only three questions. They will be functional for a while but we may change which Toolkits and Background documents have the survey functional over time. The survey opens in a new window so it can be completed after users read or explored the tool. User IP addresses are recognized so one shouldn’t be asked to evaluate a Toolkit or Background document a second time.
When asked, please say YES to the survey!
Have more feedback? You can always use the Contact Us on the PEN website.
Written by:
Beth Armour PDt MEd
PEN® Content Manager
beth.armour@dietitians.ca
PEN® Resource Managers:
Jane Bellman MEd, RD
Kerri Staden BSc, RD
jane.bellman@dietitians.ca
kerri.staden@dietitians.ca
Putting “P” value in its place
Can you remember a published health study that didn’t report at least one P-value? You’d be hard  pressed to find one. P-values are likely the most commonly-reported statistic and the one that many health professionals are comfortable with. Yet statisticians and epidemiologists report that they are the most misinterpreted and misunderstood index in biomedical research (1). In February 2016, the American Statistical Association issued a statement on statistical significance and P-values, due to their concern that the misunderstanding about P-values is contributing to the increasing “doubt about the validity of science” (2). The statement emphasizes that a P-value by itself provides limited information and that good statistical practice should incorporate a variety of ways to summarize and interpret data.
pressed to find one. P-values are likely the most commonly-reported statistic and the one that many health professionals are comfortable with. Yet statisticians and epidemiologists report that they are the most misinterpreted and misunderstood index in biomedical research (1). In February 2016, the American Statistical Association issued a statement on statistical significance and P-values, due to their concern that the misunderstanding about P-values is contributing to the increasing “doubt about the validity of science” (2). The statement emphasizes that a P-value by itself provides limited information and that good statistical practice should incorporate a variety of ways to summarize and interpret data.
“Statistical significance is the least interesting thing about the results. You should describe the results in terms of measures of magnitude –not just, does a treatment affect people, but how much does it affect them.” (Glass – Kline reference 3)
The term P-value stands for “probability value” and is defined as: “the probability that a test statistic would be as extreme as observed or more extreme if the test hypothesis were true” (4). A study reporting a result with a P-value of less than 5% (P < 0.05) means the result is considered sufficiently unlikely to have occurred by chance to justify the designation “statistically significant”. However, when we focus too much on P-values, we can miss other critical elements of the research findings such as:
- Is the P-value small because the sample size was very large? Alternatively, was the p-value large (and not “significant”) because the sample size was too small?
- Is the research free from bias?
- How confident are we that the finding is not just due to random error?
- How many statistical tests were done? Was there multiple testing?
- Does the treatment make a difference of sufficient magnitude to be important to people? (Is it clinically significant?) What is the size of the effect?
- How wide is the confidence interval and what possible results are included within it?
Why P-values can mislead us
- Sample Size
P-values are highly reliant on the study’s sample size.- A small and clinically unimportant treatment effect can be statistically significant (small P-value < 0.05) when the sample size is large.
- A large treatment effect is not likely to be “statistically significant” with a small P-value if the sample size is small.
- Bias
Flaws in how research is designed, conducted, analyzed or reported can lead to over or underestimation of the true effect of an intervention which is referred to as bias. Bias may be the actual cause for the effect observed and not the treatment. The existence of bias does not mean that the researchers meant to alter the study findings, although this can occur. Bias is more likely with some study designs (observational vs RCT) but can be introduced in careless design or conduct of any study, such as during the selection of control groups, by using randomization protocols that can allow the investigators to influence which group participants are placed in, or from lack of control of confounding variables. For more information on bias and how to assess it, see Cochrane Risk of Bias tool. - Random Error
Random error refers to the differences in results due to chance alone. By chance, some P-values are small for relationships that are not important for health. To assume that there is an important relationship because of the small p-value can be an incorrect conclusion. This error is sometimes referred to as a type 1 error, and its chance of happening is equivalent to the P-value, usually 5%. - Multiple testing
P-values are sometimes used to identify “associated” relationships in databases and when a large number of statistical tests are performed in a study. This procedure is referred to as “fishing expeditions” because many associations are tested for instead of testing pre-specified hypotheses. Sometimes studies assess dozens or hundreds of associations. In doing this, by chance alone you will find a statistically significant result because by definition, P-values <0.05 are likely to be found 5 times in 100 tests. Sometimes new and important findings are discovered through these “fishing expeditions”. However, this practice is generally frowned upon. The best practice is for researchers to only conduct a limited number of pre-determined tests to answer their research question(s).
Clinical Significance or ‘How much of an effect?
- Effect size
Whether a treatment makes an important, difference to people is a key question. To answer it, we need to examine the “effect size” of the summary statistic that estimates the differences in effect of the treatment on the particular health outcome. The effect size may be summarized as a mean or average difference, risk difference, risk ratio, relative risk, rate ratio, hazard ratio, odds ratio or other statistic. The effect size indicates whether the treatment is likely to make a difference that people would “perceive as beneficial” (4).
A clinically important effect size can be statistically significant in one study, but not in another. The clinically important difference (effect size) is the one that matters for health outcomes. To judge clinical relevance, ideally one must use health knowledge to determine if the observed difference is important and relevant to health. If a diet change altered blood cholesterol levels by 0.1 mmol/L and this was “statistically significant according to P-value, this would not be deemed as an important difference. In a case like this with a very small effect size, it would be incorrect to rely solely on statistical significance to determine the importance of the finding. If you are uncertain about what is an “important difference”, there are cut off guidelines for various effect size measurements which can help you make decisions about what effect sizes are clinically important (6).
In practice, we must also consider costs, convenience and side effects when applying research findings to clients or patients. The P-value and effect size alone are not enough for making clinical decisions.
- Confidence intervals (CI)
The width and placement of the confidence interval helps us to understand how confident we can be that a treatment makes a real difference. A confidence interval, which is often reported just after the effect size (mean or ratio of effect) in research papers, is an estimate of the range of the likely true effect of the treatment in the population of similar people to those studied (4). Usually 95% confidence intervals are used, which refers to the degree of confidence that the true effect is within the true effect range 95% of the time.
Consider:- How wide is the confidence interval?
A wide confidence interval suggests that the effect may range from a big effect to a small one or no effect at all, which does not give much confidence in the finding. In contrast, a narrow interval increases confidence that the study is providing a precise answer.
For example: Triglycerides: mean difference of 0.34 mmol/L with a 95% CI, 0.32 to 0.36 mmol/L is a narrow CI since both sides of the confidence interval are very close to the value of 0.3 mmol/L. This gives us confidence that the true effect is likely about 0.3 mmol/L. In contrast, an odds ratio = 2.8, 95% CI, 1.2 to 6.4 is an example of a wide confidence interval since the interval extends from a value that is close to the null value of 1 up to a value of 6.4. The value close to the null value suggests there may not be any effect, while the estimate of 6.4 suggests a very strong effect. The latter means that people with the exposure were over six times more likely to experience the outcome than those who were not exposed. This confidence interval would not give you confidence that you are measuring an important effect.
- Where is the confidence interval?
It also is valuable to examine whether the confidence interval boundary is close to or includes the value of no difference (also referred to as the null value). If the confidence interval boundary incorporates the null value, then you know two things:- The treatment produced results that were not statistically different (similar information as provided by the P-value).
- The results show that the treatment may have had an important effect. If the effect size suggests an important difference and the confidence interval is not close to no effect, then the treatment may make an important difference.
Note to our readers: We plan on sharing more tools to interpret confidence intervals in an upcoming PEN eNews article.
Summary
Conclusions derived from just looking at a P-value provide only a limited understanding of the research results. It is more important to ask the question: does the research show that this treatment results in an important difference?
You can learn more about the clinical importance of the treatment if you examine the effect size and confidence intervals. The effect size and confidence intervals provide more information on whether the treatment is likely to make a difference that people would perceive as beneficial and important to them.
References- Goodman S. A dirty dozen: twelve p-value misconceptions. Semin Hematol. 2008 Jul;45(3):135-40. Abstract available from: http://www.ncbi.nlm.nih.gov/pubmed/18582619
- Wasserstein RL, Lazar NA. The ASA's statement on p-values: context, process, and purpose, The American Statistician. 2016 (accessed July 2, 2017). Available from: http://amstat.tandfonline.com/doi/abs/10.1080/00031305.2016.1154108
- Kline RB. Beyond Significance Testing: Reforming Data Analysis Methods in Behavioral Research. Washington DC: American Psychological Association. 2004. p. 95. Available from: http://edhar.cas.msu.edu/readings/Kline%20Significance%20-%20ch%203%20-%20NHST%20-%20hires.pdf
- Porta M. The Dictionary of Epidemiology, 6th Ed. Oxford University Press. Oxford UK. 2014. Available from: http://irea.ir/files/site1/pages/dictionary.pdf
- Nuzzo R. Scientific method: statistical errors. Nature. 2014 Feb 13;506(7487):150-2. Available from: http://www.nature.com/news/scientific-method-statistical-errors-1.14700
- Sullivan GM, Feinn R. Using Effect Size—or Why the P Value Is Not Enough. J Grad Med Educ. 2012 Sep; 4(3): 279–282. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3444174/
- How wide is the confidence interval?
Written by:
Beth Armour PDt MEd
Tanis Fenton RD PhD FDC
Jayne Thirsk RD PhD FDC
enews@pennutrition.com
Using the PEN System – How it works
This article was originally printed in Dietetics Today, a publication of the British Dietetic Association in July, 2017. It has been adapted here with permission.
There are lots of information sources we, as dietitians, can use to help support our dietetic practice. But, finding the time to locate the specific information we need can be challenging and time-consuming! While databases such as PubMed, The Cochrane Library and TRIP are great sources of original research, systematic reviews and meta-analysis, it takes time to scroll through all the results. This is where PEN can help…
Each topic in the PEN system is collated under a ‘Knowledge Pathway’. Each 'Knowledge Pathway' is separated into different sections (similar to an online version of chapters in a text book).
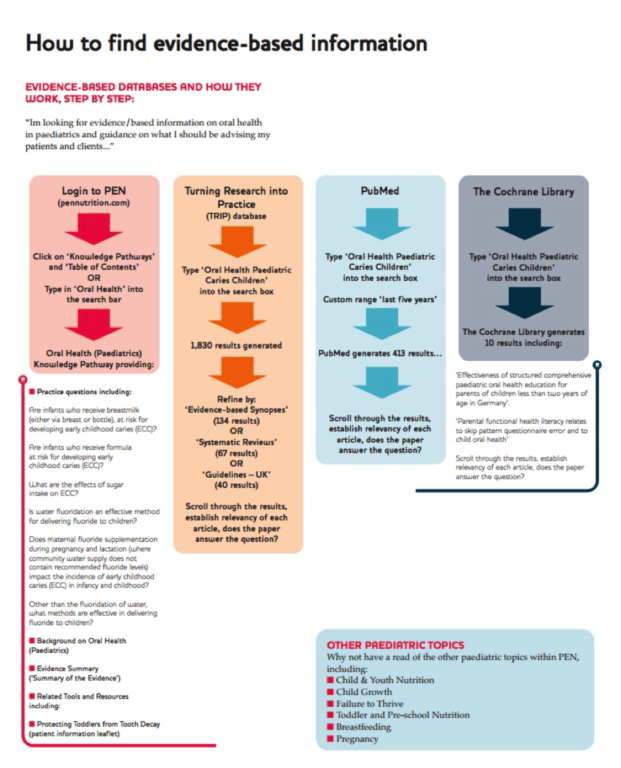
In addition to the practice questions, you can also look for:
- Practice Guidance Toolkits
- Background
- Evidence Summary
- Related Tools and Resources
The PEN System has the evidence you need at the click of a mouse!
Sammie Gill BSc (Hons), R.SEN, RD, PhD
Policy Officer (Evidence-based Practice)
British Dietetic Association
Leaky Gut Syndrome: Using PEN to debunk the myths!
This article was originally printed in Dietetics Today, a publication of the British Dietetic Association in July, 2017. It is reprinted here with permission.
The theory behind Leaky Gut Syndrome is that the tight junctions in the GI tract (which control absorption of substances) do not work properly, leading to compromised gut-barrier function and increased intestinal
 permeability. Increased intestinal permeability is associated with an increased inflammatory response. Whilst this can be present in those with specific medical conditions such as Coeliac and Crohn’s Disease or those receiving chemotherapy or radiotherapy, this is not applicable to the general healthy population.
permeability. Increased intestinal permeability is associated with an increased inflammatory response. Whilst this can be present in those with specific medical conditions such as Coeliac and Crohn’s Disease or those receiving chemotherapy or radiotherapy, this is not applicable to the general healthy population. However, increased awareness of the associations between increased intestinal permeability and ill health in specific circumstances has led many people to believe that ‘Leaky Gut Syndrome’ is a valid diagnosis.
Leaky Gut Syndrome’ is often attributed to many systemic health problems and symptoms such as joint pain, eczema, chronic fatigue syndrome and a number of auto-immune conditions. Because there are so many health conditions that can be explained by Leaky Gut Syndrome, it’s an easy diagnosis. Whereas in fact, a false diagnosis often misinforms vulnerable individuals who simply want an answer to why they’re feeling the way they are. Worryingly, the ‘treatment’ for Leaky Gut Syndrome is…you’ve guessed it…fad diets! Gluten-free and low FODMAP diets are also popular so called ‘solutions’ in addition to supplements and herbal remedies.
What is the take home message?
In a nutshell, Leaky Gut Syndrome is speculative and an unverified condition. There is no high-quality research supporting the theory of Leaky Gut Syndrome nor that it is the direct cause of widespread health problems. Have a read of the Are Your Clients Asking About "Leaky Gut Syndrome"? Trending Topic on PEN for more information and some useful links which go into more depth about the misconceptions surrounding Leaky Gut Syndrome.
Here is the next collection of Knowledge Pathways that we are planning to add or enhance in the near future.
Fructose Post Operative Chyle Leaks |
Nutrigenomics Lactose Intolerance Wound Care - Pressure Injuries |
Written by:
Sammie Gill BSc (Hons), R.SEN, RD, PhD
Policy Officer (Evidence-based Practice)
British Dietetic Association
Contact Us
Do you have comments, questions or feedback? Connect with us!



To access current and archived copies of PEN® eNews, go to: http://www.pennutrition.com/enews
Do you have comments, questions or feedback? Please contact us:
Jayne Thirsk RD, PhD, FDC
Director of PEN®
Dietitians of Canada
enews@pennutrition.com
Sammie Gill BSc (Hons), PGDip, R.SEN, RD.
Policy Officer (Evidence-based Practice).
British Dietetic Association
globalpen@bda.uk.com
Maree Hall APD
Public Relations Manager
Dietitians Association of Australia
prmanager@daa.asn.au
A Publication of the PEN System Global Partners,
a collaborative partnership between International Dietetic Associations.
Copyright Dietitians of Canada. All Rights Reserved.