PEN eNews 8(4) February 2019
PEN
® eNews is a monthly e-newsletter shared with the global PEN Community and created to help dietitians position themselves as leaders in evidence-based nutrition practice. In addition, users of the PEN System will find articles on the new evidence, resources and features available and how to maximize one's use of PEN.

A new year… take a look back and recommit to the value of PEN to practice
Each year at this time, the PEN team makes the website ready for our annual
Health on the Net (HON) recertification. We’re very proud to meet these international standards for the ethical

presentation of health information on the internet. You can read about the full HONcode on their website, but it reinforces the PEN values of providing objective, evidence-based nutrition practice recommendations and of our commitment to transparency regarding who contributes to PEN and the evidence they use. In this regard, our authors and reviewers are acknowledged on the website and each provides a declaration of interest noting any perceived conflicts of interest regarding the content they contribute to. We’ve also begun posting our search strategies so our users can be assured that we are balanced and objective regarding the evidence used to prepare the recommendations in PEN that you’ve come to rely on. Check out details of and a search strategy sample
here. While you are at it, please take a minute to learn about the
global PEN team that oversees the strategic direction for this service as well as the
PEN Advisory Committees and
hardworking staff and contractors that do the heavy lifting of finding, reviewing, synthesizing, appraising, editing, loading and curating the content as well as serving as mentors to our volunteer writers and reviewers.
Our HON recertification also means we recommit to our sponsorship policy of not allowing sponsorship or advertising in support of developing PEN System content. We rely on the revenue from subscriptions and licensing agreements to keep the content current and growing. It is complicated and time-intensive work and we appreciate every dollar we receive from our subscribers to support this work. Help us spread the word about the value of PEN and ensure its ongoing sustainability by encouraging your colleagues or employer to consider a
PEN subscription.
In this issue of PEN eNews 8(4), we:
- Share our PEN Year in Review
- Discuss the ketogenic diet
- Inform you of our new content
- Titillate you with our Trending Topics
- Tempt you with a tale of one dietitian's experience learning to be a PEN peer reviewer
- Enjoy PEN eNews 8(4)!
A Publication of the PEN® System Global Partners, a collaborative partnership between International Dietetic Associations. Learn more about PEN.
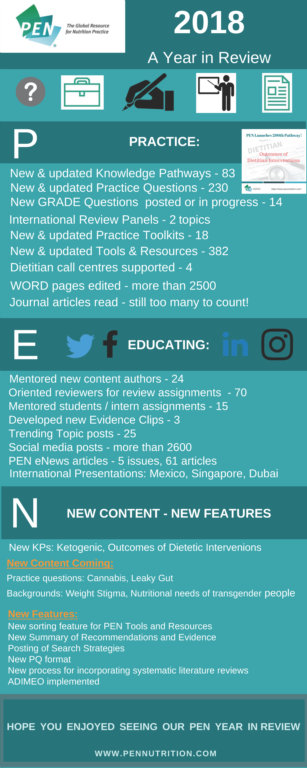
PEN Year-in-Review
We’ve summarized some of our PEN activities accomplished last year in an infographic.
Discussing our NEW Ketogenic Diet Pathway
If you conduct a Google search on the ketogenic diet it returns over 42 million results! Dietitians want to understand the evidence behind the phenomenal interest in this dietary approach.
Responding to a user request for an evidence review of the safety of ketogenic diets in pregnancy, the PEN team collaborated with the Canadian Agency for Drugs and Technology in Health (CADTH) to examine the literature in this area. See what we found at:
What is the clinical evidence describing the safety of a very low carbohydrate (20-50 g/day) ketogenic diet during pregnancy?
We were also fortunate to work with the Diabetes, Obesity and Cardiovascular Network of Dietitians of Canada on a question related to use of the ketogenic diet in weight loss.
What is the clinical effectiveness of the ketogenic diet on weight loss and cardiovascular risk factors in adults with overweight/obesity?
A further partnership will help us look at the evidence related to the use of the ketogenic diet in diabetes management using a GRADE approach. Look for that content to be posted in the PEN System in the coming months.
Following the publication of the two practice questions and the PEN Background on Ketogenic Diet, a unique exchange with our Senior Evidence Analyst Dawna Royall (DR) and Carmen Pellegrino (CP), a outpatient dietitian practicing in British Columbia, Canada, provided some additional information for practitioners exploring using the ketogenic diet with their clients. We thought it was worth sharing a couple of highlights of that dialogue with our PEN eNews audience.
DR: Thanks for your interest in the ketogenic diet knowledge pathway in PEN.
First of all, I'd like to emphasize that there is limited research evidence to answer some of your questions. While we appreciate that practitioners have experience and opinions regarding treatment and monitoring of individuals on the ketogenic diet, we have limited the information in PEN to that which is supported by the peer-reviewed literature.
CP: Please explain which labs should be focused on for the Keto Diet, if any?
DR response: Monitoring urine ketones is important to ensure that the diet is being managed correctly. Blood lipids should be monitored given the potential effect of the diet on blood lipids, in addition to blood glucose and standard measures of nutrition assessment. There is a recent narrative review by Gupta et al. (1) that provides some practical information about the ketogenic diet, but I caution you that it is a narrative review and there is no search strategy or quality assessment of included studies to support the information. The authors suggest the following monitoring, but do not provide a reference to support the suggestion: "It is generally advisable that patients on KD should monitor their serum glucose, albumin, total protein, total cholesterol, triglycerides, and serum creatinine once in every 3 months. Once a year, renal ultrasound, bone density, carnitine, selenium levels, and electrocardiogram are significant with regard to the prevention of long-term effects such as nephrolithiasis, osteoporosis, hyperlipidemia, carnitine deficiency, and cardiomyopathy." (1)
CP: What are specifically the micronutrient deficiencies that could develop. I'm aware 'B' vitamins because of the lack of whole grains/starches. If there are any additional harms/dangers, please elaborate.
DR response: In the PEN background document we identify that "Nutrients of particular concern on the ketogenic diet are calcium, vitamin D, selenium, magnesium, zinc and phosphorus".
CP: Are there any studies on the ketogenic diet that follow subjects for longer than 1 year?
DR response: The systematic review by Bueno et al. (2) that we cite in the PEN question included 4 studies that followed participants for 2 years. Unfortunately, in these 4 studies (similar to the 1-year studies), compliance was poor* so that mean carbohydrate intake for participants at the end of the follow-up period was either unreported or carbohydrate intake was 40-47% of energy intake, which we know is no longer a ketogenic diet. There were no other long-term studies identified in the literature related to this question (effect on weight loss and CV risk factors for individuals with overweight / obesity).
CP: Why isn’t the pH in blood decreasing in ketogenesis as it is during diabetic ketoacidosis. and how are ketone bodies kept under control and within safe limits?
DR response: The PEN Background provides some details on the biochemistry at work in both ketosis versus diabetic ketoacidosis. Paoli et al. (3) also provides a good overview of physiological ketosis although it is not a systematic review of the evidence for health effects of the diet. In diabetic ketoacidosis, accelerated ketosis occurs due to increased gluconeogenesis so that the ketone bodies cannot be used for energy to the extent that they are produced, resulting in extremely elevated blood sugars and acidic pH. With long-term starvation (or the equivalent as achieved by a ketogenic diet), endogenous insulin protects against the occurrence of diabetic ketoacidosis; ketone levels in the blood do not exceed 7-8 mmol/L because they are efficiently used as a source of energy.
References:
- Gupta L, Khandelwal D, Kalra S, Gupta P, Dutta D, Aggarwal S. Ketogenic diet in endocrine disorders: Current perspectives. J Postgrad Med. 2017 Oct-Dec;63(4):242-51. doi: 10.4103/jpgm.JPGM_16_17. Abstract available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5664869/
- Bueno NB, de Melo IS, de Oliveira SL, da Rocha Ataide T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. Br J Nutr. 2013 Oct;110(7):1178-87. doi: 10.1017/S0007114513000548. Epub 2013 May 7. Abstract available from: https://www.ncbi.nlm.nih.gov/pubmed/23651522
- Paoli A, Rubini A, Volek JS, Grimaldi KA. Beyond weight loss: a review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur J Clin Nutr. 2013 Aug;67(8):789-96. doi: 10.1038/ejcn.2013.116. Epub 2013 Jun 26. Abstract available from: https://www.ncbi.nlm.nih.gov/pubmed/23801097
Revisiting Trending Topics
In this issue of PEN eNews, we wanted to highlight our
Trending Topics f

eature. Some of you may not be familiar with this feature and so we thought that by sharing some highlighted ones from the past couple of months we can demonstrate how this section in PEN can help you stay on top of key nutrition controversies, new research and complement the more detailed analysis you see in the PEN pathways. Trending Topics can be searched by using the
Popular Tags.
Food Sensitivity Tests
A recent
ar ticle
ticle was published by CBC Marketplace about the misuse and misinterpretations of IgG tests for food intolerance. The article notes that medical experts, including the Canadian Society of Allergy and Clinical Immunology (CSACI), call IgG tests for food sensitivities “unvalidated,” and more than two dozen organizations warn about the misuse of such tests. Related information will be updated in the
Food Allergies Knowledge Pathway soon.
Family Meals and Teen Diets
 Teens Who Eat Meals with Family 'Have Healthier Diets'
Teens Who Eat Meals with Family 'Have Healthier Diets' is a recent Behind the Headlines posting from the National Health Services (NHS) in the U.K. Research was conducted at the University of Guelph in Canada; Amherst College, Harvard Medical School and Brown University in the U.S.; and Loughborough University in the U.K. The study results showed, "not only do families with lower levels of family functioning participate in frequent family meals, but that family dinners are associated with improved dietary intake, regardless of level of family functioning". See Additional Content:
Healthy Lifestyle - Eating Together Knowledge Pathway. Watch for updates to this PEN
® content soon.
Probiotics in the News
.jpg)
There is a lot of attention in social media lately about recent studies related to probiotics. The International Scientific Association for Probiotics and Prebiotics (ISAPP), which is an international group of probiotic scientists, provides critique of these studies.
Click here for details.
Further Commentary on the PURE Study: Dairy Intake, Cardiovascular Disease and Mortality
An editorial by Louie and Rangan discusses the findings from the Prospective Urban Rural Epidemiology (PURE) study on the association of total and individual types of dairy food intake with major cardiovascular disease events and mortality (1). The editorial authors report that the PURE study found that higher daily consumption of dairy products may be protective and that the associations were stronger for whole fat dairy foods in low and middle income countries with lower mean dairy intakes (i.e. South and Southeast Asia, Africa and China).
Louie and Rangan point out that while this current analysis is not as affected by the study design issues of other PURE study results, there were large limitations; the most notable being that dietary intakes were only assessed at the beginning of the study (1). A single assessment of dairy consumption may not be an accurate reflection of intakes over the course of the nine years of follow up and this reduces the certainty of the findings. The authors caution that readers should consider this study as only another piece of the evidence, and strong recommendations cannot be made for the consumption of higher fat (versus lower fat) dairy products. The study’s results only suggest that the consumption of dairy products may be encouraged for low and middle income countries and dairy products should not be discouraged for other consumers.
For additional discussion of the PURE study findings, see the PEN Trending Topic: Dairy Intake, Mortality and CVD – The Debate Continues.
Reference
- Louie JCY, Rangan AM. No need to change dairy food dietary guidelines yet. Lancet. 2018 Nov 24;392(10161):2242-4. doi: 10.1016/S0140-6736(18)31945-7. Epub 2018 Sep 11. Citation available from: https://www.ncbi.nlm.nih.gov/pubmed/30217461
Update on the Mediterranean Diet
How does the retraction and republication of the PREDIMED trial affect recommendations for a Mediterranean diet? The related PEN content was reviewed and updated accordingly:
Recommendation
The Mediterranean dietary pattern is recommended to lower the risk of cardiovascular disease (CVD).
Grade of Evidence B
Updated Evidence
A clinical trial from Spain (PREDIMED study) was retracted due to irregularities in the randomization procedures that included enrolling participants who were not randomized. In the PREDIMED trial, participants were randomized by advice to follow a Mediterranean (Med) diet supplemented with extra-virgin olive oil (50 g/4 Tbsp/day), a Med diet supplemented with nuts (30 g/day walnuts, hazelnuts and almonds) or a control, low fat diet. The study was reanalyzed by excluding participants (n=1588) who deviated from the randomization protocol; republished results did not change the overall results (1). After a follow up of five years, a 29-32% reduction in major CVD events (composite of myocardial infarction, stroke, or CVD mortality) was reported in both of the Mediterranean diet groups compared to the control. When the 1,588 participants were excluded from the analysis, the risk of major CVD events was: Med diet + olive oil group (hazard ratio (HR) 0.71; 95%CI, 0.52 to 0.97); Med diet + nuts (HR 0.68; 95% CI, 0.49 to 0.95). For individual components, only stroke risk was significantly reduced (Med diets combined HR, 0.58; 95%CI, 0.42 to 0.82). Effects on blood lipids were not reported.
For additional information, see the PEN Practice Question: In adults with elevated LDL-cholesterol (LDL-C), what are the effects of dietary patterns (i.e. Portfolio, Mediterranean, DASH) on LDL-C levels?
Reference
- Estruch R, Ros E, Salas-Salvadó J, Covas MI, Corella D, Arós F, et al.; PREDIMED Study Investigators. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N Engl J Med. 2018 Jun 21;378(25):e34. doi: 10.1056/NEJMoa1800389. Epub 2018 Jun 13. Abstract available from: https://www.ncbi.nlm.nih.gov/pubmed/29897866
Just What Did the VITAL Results Teach Us About Vitamin D and Omega-3 Supplementation?
The Vitamin D and Omega-3 Trial (VITAL) was a very large randomized placebo-controlled study (with a two-by-two factorial design), which examined the effects of vitamin D or omega-3 supplementation on the primary outcomes: major cardiovascular (CV) events (myocardial infarction (MI), stroke, CV-related death) and invasive cancer (1,2). The study included 25,871 participants, 50 years or older for men and 55 years or older for women (20% of whom were black as prespecified in the study design). Participants were given 2000 IU/day vitamin D3 and 1 g/day of marine omega-3 fatty acids (either alone or in combination) or placebos. After five years, neither supplement resulted in significantly lower incidences of the primary outcomes, major CV events or invasive cancer, compared to the placebo. The outcomes were confirmed using medical records.
The bottom line is that neither vitamin D nor omega-3 fatty acid supplements lower the incidence of any invasive cancer or reduce major CV events. Further research is needed to determine if omega-3 fatty acids have any positive influence on reducing MIs among black people (a secondary finding).
Secondary Findings
In this study, researchers also looked at several other outcomes (MIs, stroke, cardiovascular deaths and deaths from any cause), which were considered secondary analyses (1,2). While most of these secondary analyses also suggested no benefits from either of these supplements, one of the observed secondary results might suggest that there could be a beneficial effect (lower risk of MI (HR, 0.72; 95%CI, 0.59 to 0.90) with supplementation of omega-3s (particularly in black participants (HR, 0.23; 95%CI, 0.11 to 0.47)). While this sub-analysis is interesting, it was not specified as a primary outcome at the start of trial, so it is possible that this statistical significance is due to chance alone. When many statistical tests are conducted, the probability of finding positive results increases with each additional test. Before secondary analyses should be considered to have any validity, they need to be tested as primary endpoints in adequately powered RCTs.
To assess whether the secondary result might suggest a benefit, it is important to examine its numerical value. The magnitude of the results for the overall reduction in MIs was (0.72 (95%CI, 0.59 to 0.90)) with supplementation of omega-3s. While this is statistically significant (the confidence interval did not include the null value of 1), the magnitude of the hazard ratio was greater than 0.5, a value that is considered to show a sufficient magnitude of change in health outcomes to represent an important difference (3). Using this metric, the secondary finding of reduced MIs among the black people supplemented with omega-3s (HR, 0.23; 95%CI, 0.11 to 0.47) suggests that it might be worth examining as a primary outcome in a subsequent study and the result for non-Hispanic white people suggests no effect at all of omega-3s on MI risk (HR, 0.93; 95%CI, 0.73 to 1.18).
For further discussion on the findings, see:
Vital Signs for Dietary Supplementation to Prevent Cancer and Heart Disease (Editorial)
VITAL: No CVD or Cancer Benefit from Vitamin D, Omega-3 (Free Membership Required to Access).
See PEN® Practice Questions:
Are vitamin D and/or calcium supplements recommended for prevention or treatment of cardiovascular disease (CVD)?
Should omega-3 fatty acids (fish or plant-based food or supplements be recommended for the primary or secondary prevention of cardiovascular disease (CVD) in adults?
References
- Manson JE, Cook NR, Lee IM, Christen W, Bassuk SS, Mora S, et al.; VITAL Research Group. Vitamin D supplements and prevention of cancer and cardiovascular disease. N Engl J Med. 2018 Nov 10. doi: 10.1056/NEJMoa1809944. [Epub ahead of print]. Abstract available from: https://www.ncbi.nlm.nih.gov/pubmed/30415629
- Manson JE, Cook NR, Lee IM, Christen W, Bassuk SS, Mora S, et al.; VITAL Research Group. Marine n-3 fatty acids and prevention of cardiovascular disease and cancer. N Engl J Med. 2018 Nov 10. doi: 10.1056/NEJMoa1811403. [Epub ahead of print]. Abstract available from: https://www.ncbi.nlm.nih.gov/pubmed/30415637
- Guyatt GH, Oxman AD, Sultan S, Glasziou R, AKL EA, Alonso-Coello P, Atkins D, et al. GRADE guidelines: 9. Rating up the quality of evidence. J Clin Epidemiol. 2011 Dec;64(12):1311-6. Abstract available from: https://www.ncbi.nlm.nih.gov/pubmed/?term=21802902
Giving back - My experience of becoming a peer reviewer for PEN
Whilst reading Dietetics Today, I came across a call for Dietitians  to apply to become PEN reviewers. As I have gleaned so much valuable and relevant evidence-based information from the PEN site, I thought it time to give something back. So, I applied and was accepted, which was heartening!
to apply to become PEN reviewers. As I have gleaned so much valuable and relevant evidence-based information from the PEN site, I thought it time to give something back. So, I applied and was accepted, which was heartening!
I was given a choice of topics and selected Healthy Eating as one and Rheumatoid arthritis as the other.
As a PEN Reviewer, you are expected to review the new or updated PEN content by completing the relevant searches to ensure the evidence presented is accurate. If you have a lot of experience, you may be aware of the evidence anyway and this really helps with time management, but I love seeking out evidence and this is not a burden to me anyhow.
The process is fairly clear and your role as a reviewer is to do just that – to review the evidence and the text of the information for accuracy and ease of understanding. As you should already know (!) the evidence is divided into practice questions with key practice points, practice guidance and grading of the evidence. The reference list is also provided at the end of the guidance
My favourite part of the process was looking at the evidence. I have a lifelong curiosity about research which improves patient care and doing the reviews enabled me to both indulge this curiosity as well as expand my own knowledge base.
The process was not to too demanding time wise and I think it really beneficial to have a deadline to work to as this means that there is a start and finish which certainly kept me focused. I would estimate that each review took me about 4 hours, but I think this depends upon your familiarity with the subject. But I would also suggest that to review a subject outside your comfort zone is good for your professional and personal development!
The policy officer responsible for the administration of the work was very helpful and I used a previous completed guideline, complete with tracked changes, as a steer. This was enormously helpful.
I am now really looking forward to undertaking more work
My tip for anyone thinking of becoming a reviewer is to jump in the deep end and have a go. Choose a simple topic with which you feel comfortable (sorry, but I have done the healthy eating review !!!) and take time to read the content before you begin. Get hold of a copy of a completed review so that you have a clear idea of a) what is expected and b) what detail is expected.
I am sure that if you want some support to help you gain confidence to the work well, mentors such as myself would be only too happy to provide support.
There is also the opportunity to write new guidance, especially if you have done a piece of work for which there is limited content on PEN or elsewhere.
PEN succeeds entirely because Dietitians are willing to develop and review the content. Without us I guess it would not exist.
Be like the old NIKE advert – just do it!
Sue Acreman RD FBDA MSc
Freelance dietitian, previous member of Council, two-time Chair of the SW branch of the British Dietetic Association (BDA), a trustee of GET and a Fellow of the BDA
Contact Us
Do you have comments, questions or feedback? Please contact us:
Jayne Thirsk RD, PhD, FDC
Director of PEN®
Dietitians of Canada
jayne.thirsk@dietitians.ca
Eleanor Johnstone PG Dip, BSc, RD
Policy Officer (Evidence-based Practice).
British Dietetic Association
globalpen@bda.uk.com
Sally Moloney APD
Public Relations & Marketing Manager
Dietitians Association of Australia
pr@daa.asn.au
PEN eNews
February 2019 Volume
8 (4)
A Publication of the PEN® System Global Partners,
a collaborative partnership between International Dietetic Associations.
Learn more about PEN.
Copyright Dietitians of Canada
. All Rights Reserved.